Review of Rebecca Onie What if Our Healthcare System Kept Us Healthy
Overview of the American Healthcare System

Introduction
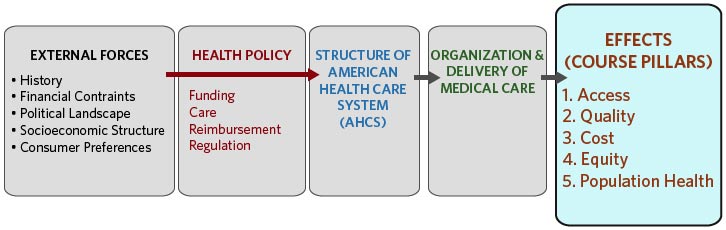
External forces of history, fiscal constraints, political mural, current socioeconomic structure and consumer preferences shape the structure, or lack thereof, of the American wellness care system—often through health policy decisions nearly funding care, reimbursement, and regulation. Direct effects can exist seen in the arrangement and commitment of care. A focus of our class will be the downstream effects on access, quality, price, equity, and population health. These five elements of health care are the pillars of this course.
The Usa has the trifecta of high price, unequal access, and often below boilerplate outcomes compared to other highly developed nations. This module volition provide an introduction to the American wellness intendance system (AHCS), explore some of the complexities of wellness care delivery, and provide a glimpse of the historical evolution of the AHCS that has led to the great argue and need for health care reform today. We will differentiate between the traditional main intendance and hospital-based paradigms and more preventive, out-patient and medical home community models.
Explore the infograph about US Health Care Costs by reviewing "Visualizing Health Policy" from the September 2012 upshot of Journal of the American Medical Association. As you read, note the following:
- Increase in health care spending exceeds growth of US economic system
- Minor proportion of population uses most of resource
- Burden of health care costs on families
- Health care spending per capita in U.s.a. compared to other countries
Learning Objectives
- Identify and define the 5 course pillars.
- Describe major characteristics of the uninsured in the The states pre-implementation of changes from the Affordable Care Act (ACA).
- Distinguish between the elements of access in health intendance: access to insurance coverage, admission to services, use of services.
- Identify central terms in health care expenditures and demonstrate ability to match categories to actual data tables.
- Categorize cost containment strategies as price controls and utilization.
- Describe the electric current situation in US health care of high costs with poor outcomes and brainstorm to relate to course pillars.
- Relate a current consequence to course concepts in written form.
Health and Affliction
As we motion through the readings and ameliorate understand the foundations of the American wellness care system, nosotros are reminded that social and institutional values and behavior that emphasized affliction more wellness and prevention contributed to our astronomical costs and slowed down our progress toward attainment of a manageable and affordable system. Before nosotros continue, let's review a few conceptual health care models so that nosotros are all on the same page.
Disease
| Disease
|
How much of our poor health outcomes in the United States are due to wellness intendance. That depends on how you define health care. Watch Rebecca Onie's TED Talk below. What type of services do you think should be incorporated into health care settings.
TED Partner Series Rebecca Onie: What if our healthcare system kept us healthy?
Filmed April 2012 • Posted June 2012 • TEDMED2012
The American Health Intendance System
Wellness Care CommitmentThe Us is amongst the wealthiest nations in the earth, but information technology is far from the healthiest. Although Americans' life expectancy and health have improved over the past century, these gains accept lagged behind those in other high-income countries. This health disadvantage prevails even though the U.s.a. spends far more than per person on health care than whatever other nation. Institute of Medicine. (January 2013). REPORT Brief U.S. Health in International Perspective: Shorter Lives, Poorer Health | |
| | "Making systems work is the great task of my generation of physicians and scientists. But I would go farther and say that making systems work — whether in healthcare, education, climate change, making a pathway out of poverty — is the great task of our generation as a whole." Atul Gawande: How do we heal medicine?- TED Talks 2/2012 |
| | "There are also many examples that show how our arrangement can fail to run into patients' needs. These issues are not a reflection on the many doctors, nurses and other professionals who piece of work tirelessly to deliver the highest quality care they can. Instead, they reflect a commitment organisation that'south not ever designed with the patient in listen." Donald Berwick, Former Manager of the Centers for Medicare and Medicaid Services 7/iii/2011 |

What is the wellness care system? What is the medical care system? Are they systems? In this course we volition discuss the AHCS as if information technology were a unified structure. At the same time we will point out the many ways in which it is not.
Medical care is ofttimes understood as the more than clinical aspects that take place in the traditional medical setting.
Health is a much broader concept. The wellness intendance arrangement extends far beyond the examination room and we will come across this in upcoming week.
For the purposes of this course we will use the term AHCS to refer to health services, health care delivery, public health, and traditional medical care
The following table gives you an idea of the complexities of health intendance commitment in our land. Note that it is divided into organizations (pedagogy/enquiry and or managed care/integrated networks), individual suppliers, insurers, providers, payers, funders, and—final but not least—the government. We will be discussing all of these components over the course of this semester, and then continue this nautical chart handy.
The American Health Care System as a Non-Organization
Though the American wellness care system is a far cry from being a well-oiled automobile, information technology does have various components that are interdependent and share mutual goals. These components exercise fit into a systems model, despite all its limitations. Shi and Singh use this systems framework to illustrate some bones foundations that back up the interaction between input (resources) and output (outcomes), likewise as the underlying structure that supports the process dynamics, which evolve over fourth dimension.
Surely, the American wellness care system is far from perfect, but, then, by now you probably realize that no perfect organization exists anywhere. Americans have access to a patchwork of subsystems (like managed care, the Veterans Administration, and emerging IDSs) that characterize health intendance delivery in the US. Notwithstanding, the systems framework does requite u.s. at least a starting identify to try in an organized mode to understand an extremely convoluted, confusing, and costly health care system, and perhaps, a place to begin our quest to find acceptable solutions to our problems.
Atul Gawande is a surgeon and writer from the Boston area. Watch the video beneath for an academic and clinical perspective on our cleaved medical care systems. Focus in detail, to the questions below:
- What does he mean when he says this is non a system?
- What are the 3 steps for making systems work?
- Who are the cowboys?
- Who are the pit crews?
Atul Gawande: How practise we heal medicine?
Consider the data taken from the beginning chapter of a recent IOM study entitled All-time Care at Lower Cost: The Path to Continuously Learning Health Intendance in America:
- If shopping were similar health care, production prices would not be posted, and the cost charged would vary widely inside the same shop, depending on the source of payment.
- If automobile manufacturing were like health care, warranties for cars that crave manufacturers to pay for defects would non exist. Equally a outcome, fewer factories would seek to monitor and better production line performance and product quality.
- If airline travel were like health intendance, each pilot would exist free to design his or her own preflight safety check, or not to perform ane at all.
Access
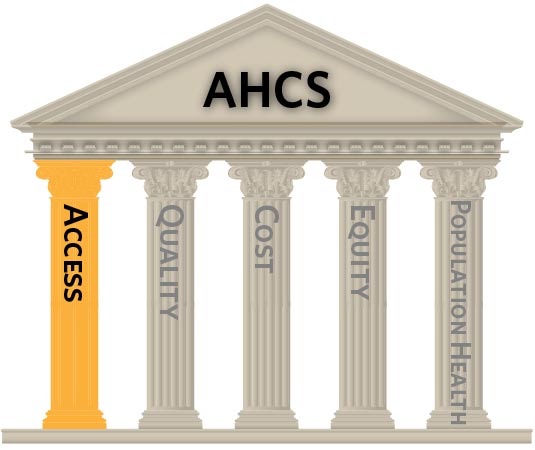
Access, Quality, Cost, Equity, and Population Health are the five pillars of this form. We will introduce these concepts today with an emphasis on access.
What is Admission?
Admission in health intendance refers to the power of individuals to obtain needed services.
Healthy People 2020 described iv components of wellness services access.
Coverage
- Health insurance does not guarantee admission, simply it facilitates entry to health intendance services.
- In 2012 at that place were about 47 meg non-elderly people without insurance. Why exercise we say non-elderly? Considering Medicare coverage of the population 65 years and older provides a loftier level of coverage not seen in other age groups. It is important to think this when thinking nigh insurance coverage and the uninsured.
- Rates of uninsurance are a moving target, particularly with the January 2014 implementation of the ACA private mandate, Medicaid expansion (in some states) and opening of the Exchanges for private plans. See below.
The Affordable Intendance Deed (ACA) includes elements of insurance coverage through individual mandates, employer mandates (postponed until 2015) , health insurance exchanges, subsidies for low-income Americans and Medicaid expansion (only in some states) for those in poverty are intended to increase access.
We will return to the topic of Medicaid expansion in u.s.a..
Services
- Ideally admission would starting time with continuity of care from a primary intendance provider (PCP).
- It is less than ideal when the source of non-emergency intendance is in the emergency section.
- We volition encompass many of the other wellness care providers and intendance settings equally the semester continues.
Timeliness
- Timeliness encompasses waiting fourth dimension at indicate-of-care commitment, and lag time between the decision to access a service and the bodily receipt of that service.
- Timeliness is also an important aspect of quality.
Workforce
- The shortage of PCPs in the US threatens admission, quality and price.
- Increased use of mid-level practitioners (PAs, NPs) is seen as a potential solution.
- Innovating service models such every bit telemedicine and team models for primary care may also expand the reach of our existing workforce.
How practise we evaluate admission?
Measures of access to care may be private or population based. These include the following:
- Identification of a usual source of care
- Report of going without intendance due to cost
- Receipt of preventive care (immunizations, colonoscopy)Insurance coverage
- Dental visit inside 1 year
- Expect time to side by side appointment
- Preventable hospitalizations
- Time or phase at diagnosis for cancer
- Excess deaths (those thought to be preventable through medical care)
The data for several of these measures came from the perspective of patients. When examining access from utilization remember that you are only capturing those who were able to get care. Think virtually the measure out for 'percent of patients with lower dorsum pain receiving an MRI.' If this is based on a review of records for lower back hurting patients you only capture those people who chose to or were able to get services in the get-go place. This measures the rate of MRI apply for dorsum hurting in a clinical setting, non in the population.
The Uninsured
Throughout the semester we will use materials from the Kaiser Family Foundation (KFF) and the associated sites Kaiser Health News for current events, and KaiserEDU for wellness policy information.
Note: the Kaiser Family unit Foundation is a not-for turn a profit foundation focusing on wellness policy, wellness journalism, and advice. There is no relationship with Kaiser Permanente or Kaiser Industries.
As we finish upwardly on access please bank check to see how much yous know about the uninsured in the U.S using the Uninsured Quiz from KFF. This is a tool for self-assessment and does not gene into your class. Resist the urge to look upwardly the answers! At the end of the quiz you lot will be able to view your responses, the correct answers with feedback, and links for further information.
 | The large number of uninsured people in the U.s. has been at the forefront of health policy discussion for decades, and in recent years has received increased attending with the passage of the wellness reform law in 2010. How much do you know about the uninsured population and the consequences of not having coverage? Take the quiz below to find out. |

Quality and Cost
Quality
The Institute of Medicine defines quality as "the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with electric current professional knowledge".
The primal components for admission to quality care:
- Safe
- Timely
- Constructive
- Efficient
- Equitable
- Patient-Centered
This data comes from the IOM 2001 written report Crossing the Quality Chasm: A New Health Organization for the 21st Century.At that place is much more to say virtually quality in health care. You could spend your career on this topic and still take more to learn. Quality will exist a recurring theme, and we will return specifically to quality, evaluating quality, and quality comeback initiatives later in the semester.
Cost
Why do we care so much well-nigh cost? Because 17.2% of our spending in 2012 as a nation was on health-related expenditures. Wellness care costs are increasing faster than wages, which means that an increasing proportion of household income is spent on health care (premiums and out of pocket). If health care spending crowds out other spending priorities on the national or individual footing we accept a trouble. Are we spending as well much? That depends on your perspective and spending priorities.
National Health Expenditures: total amount spent for all heath services, wellness inquiry and related construction activities for one calendar twelvemonth.
- Categories of spending: personal health intendance (spending for medical weather on individuals), government public wellness activity, government administration and internet cost of health insurance (turn a profit or loss of insurance companies) and investment (noncommercial research, structures, equipment).
- NHE may also be broken down by source of funding: consumer out of pocket, private health insurance, Medicare, Medicaid, and other spending by state or federal authorities).
Gross Domestic Profit (Gdp): Summary measure of the economy, could be measured in a few ways. Consider this to be how much is spent in the US on everything, including healthcare.
PDF File
| U.s.a. Annual Health Expenditures Matching Do |
| In the matching practise below, match the categories of expenditure with the numbers and dollar expenditures. You can use this file on US National Wellness Expenditures to assistance you.. |
| |

Important Principles for Understanding Costs in Wellness Care

Total price = price of service ($) ten number of services provided
Total cost for MRIs = cost of each MRI x number of MRIs for your customers
What if you are in accuse of buying coffee for the role? You have a automobile and each loving cup costs the company $two. If you provide an unlimited number of k-cups there is no limit to how much you will have to spend (fee for service) method for reimbursing providers for each unit of service provided. If you put out a certain number per mean solar day you will limit the number of cups (volume), but y'all may not accept an equitable distribution across co-workers (rationing) equitable distribution of limited resource. You could charge your co-workers a small-scale fee per serving (cost sharing). How practise you best allocate your resources (funds to buy java) across the grouping?
Now let'south go to health care. You are an insurance company and you would like to spend less on MRIs adjacent year. How do y'all save coin? Yous lower the price (price) by negotiating a amend rate with an MRI vendor. Maybe you have to enter into an exclusive contract or hope a certain patient volume. Yous could charge patients for each examination that reduces the insurance company'south cost. Bottom line is that you pay less per test. You lower the volume by non paying for as many MRIs. Y'all could require a (prior approval) requirement that provider seek approval from insurance company before providing wellness care services to ensure that payer volition cover the expense process. Some providers may non order as many MRIs if your process is a hassle. You could increase the patient portion of the nib (cost sharing). Some patients may not be able afford this and skip the test. You could merely not cover MRIs for certain diagnoses.
If you want to save money for wellness services you demand to use less expensive services (pay less, or a cheaper service) or you tin apply fewer services. Call up about access. Does expanding access salve money? Not at the beginning. If you requite people insurance they will likely use services.
ii. Whose cost are you talking about?
Providing wellness insurance may relieve money for the newly insured. Maybe he or she at present has coverage for something that used to exist an (out of pocket expense) amount of money that patient pays for health intendance services excluding premiums. This is individual cost.
If yous first to provide coffee at work you lot could save money for your co-workers considering they volition no longer go across the streets and pay for a cup. This is an case of (cost shifting).
3. Is cost all nigh money?
Non at all, just that will be our focus when we talk most costs this semester.
In real life there are time costs (buying coffee at the market, making it, walking to the shop) that may make one of these options more or less attractive. Maybe the store java is better than what you tin can make. Information technology is more expensive, but it could have more than value for your dollar if you gene in taste.
Nosotros are just talking virtually fiscal cost so y'all are spending more if you don't make the coffee yourself. You are spending more if you don't limit how much 'complimentary' coffee your co-workers tin can drinkable.
In health care the non-fiscal toll can exist priceless: time, transportation, decreased work productivity, missed piece of work, pain, quality of life, even death.
Future Management
Can we increase access to care without increasing toll to the organisation? Not in the short term, but in that location could be longer-term payoffs.
Tin we increase quality without increasing costs to the system? Hopefully, yeah. This is a growing interest expanse for providers and researchers. How to we go the near value from our heath care resources.
There is a recognized need for change. The organisation is fragmented. Costs continue to rise. Overall, increased costs are not leading to improved health outcomes.
![]()
The IOM consensus written report (2012) Best Care at Lower Cost: The Path to Continuously Learning Wellness Care in America highlights the challenges to our electric current organization, and also describes some solutions. This post-obit infographic presents the committee's goals for the AHCS.
Equity
Improving health equity requires eliminating wellness disparities and improving health condition for the population.
Wellness Equity
Health equity is attainment of the highest level of wellness for all people. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and healthcare disparities.
National Health Disparity
A particular blazon of health difference that is closely linked with social or economic disadvantage. Health disparities adversely affect groups of people who have systematically experienced greater social and/or economical obstacles to wellness and/or a make clean environment based on their racial or ethnic group; organized religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation; geographic location; or other characteristics historically linked to discrimination or exclusion.
National Partnership for Action to End Health Disparities
Population Health
In the words of Dr. Steven Schroeder in 2007 in the assigned piece titled, Nosotros Can Practice Ameliorate — Improving the Health of the American People.
The two-part answer is deceptively simple — beginning, the pathways to ameliorate health do not generally depend on better health care, and second, fifty-fifty in those instances in which health intendance is important, too many Americans do not receive it, receive it too tardily, or receive poor-quality care." N Engl J Med 2007;357:1221-8.
Fast forrard to today and few things have inverse. In comparing to other highly developed nations we exercise poorly on many measures, especially for persons under age 50 years.
- Prevalence of specific illness
- Self-rated physical and mental health
- Quality of life
- Functional condition
- Life expectancy
- Age-adjusted decease rates
- Infant mortality rates
- Low nativity weight rates
- Cancer by stage at time of diagnosis
- Lower extremity amputations due to diabetes
- New infections with HIV
- Deaths involving alcohol or illicit substances
- Overweight and obesity
- Deaths of adolescents from guns
Consider the following ii graphs that depict the causes of death of women and men in the U.Due south. before the age of 50, compared to peer countries.
| | |
| Source: U.S. Health in International Perspective: Shorter Lives, Poorer Health | |
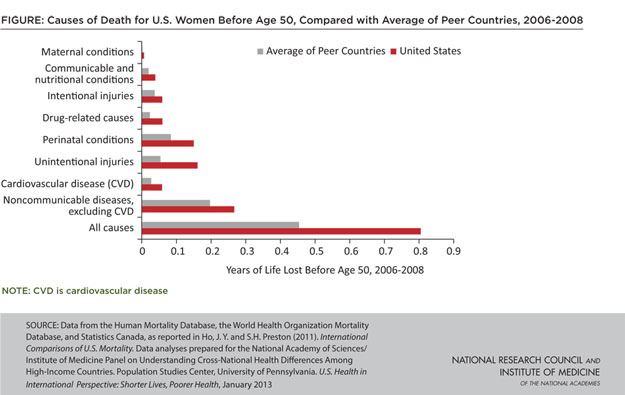
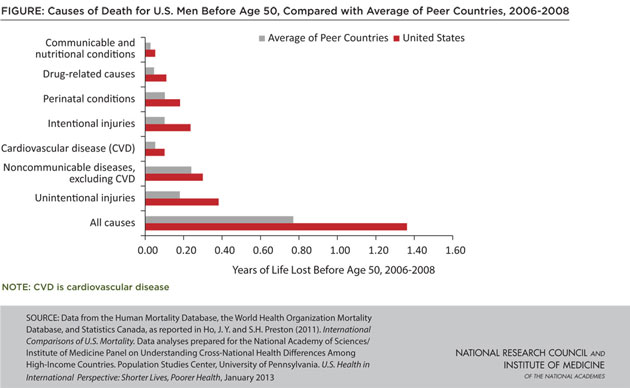
The contempo Establish of Medicine publication United states Heath In International Perspective: Shorter Lives. Poorer Health described how Americans have worse health status and die before than peers in other nations. Income is known to be linked to poor health, simply does not account for the differences. Persons with low income do worse, but when you compare within income groups we are still sicker and dice sooner.
Retrieve About These Issues Throughout the Course
There is a recognized need for change. The system is fragmented. Costs continue to rise.
Overall, increased costs are not leading to improved wellness outcomes.
Can nosotros increase access to intendance without increasing cost to the organisation? Non in the short term.
Can we increment quality without increasing costs to the arrangement? Hopefully, yes. This is a growing interest area for providers and researchers. How practise we get the nearly value from our heath care resources.
How do we tackle health disparities given the known socio-economical barrier to access to care?
davidsonengropose.blogspot.com
Source: https://sphweb.bumc.bu.edu/otlt/MPH-Modules/HPM/AmericanHealthCare_Overview/AmericanHealthCare_Overview_print.html
0 Response to "Review of Rebecca Onie What if Our Healthcare System Kept Us Healthy"
Post a Comment